÷ирроз печени
¬.≈. —иницын, ƒ.¬. ”стюжанин
ќтдел томографии »нститута кардиологии им. ј.Ћ.ћ€сникова – Ќѕ ћ« –‘, ћосква, –осси€ 3-€ „ерепковска€ ул, 15а, E-mail: ust@tomography.ru
–Я–∞—Ж–Є–µ–љ—В
–Т–Њ–Ј—А–∞—Б—В: 27 лет
–Я–Њ–ї: –Љ—Г–ґ—Б–Ї–Њ–є
–Р–љ–∞–Љ–љ–µ–Ј
ѕациент был амбулаторно направлен в наш центр дл€ проведени€ “ и ћ–“ исследований. ∆алобы на боль в животе, повышение температуры, тахикардию. ѕ€ть лет назад пациент перенес вирусный гепатит ¬.
–Т—Л–њ–Њ–ї–љ–µ–љ–љ—Л–µ –Є—Б—Б–ї–µ–і–Њ–≤–∞–љ–Є—П
“ проводилась на спиральном компьютерном томографе в односрезовом режиме, толщина среза 10 мм, без контрастного усилени€. ћ–“ проводилась на 1-“л ћ– томографе с помощью “1- и “2-взвешенных импульсных последовательностей спин-эхо, турбо спин-эхо, FLASH, а также проводилась двумерна€ ћ– флебографи€ (последовательность FLASH), толщина срезов 8 мм, без контрастного усилени€.
–Ю–±—Б—Г–ґ–і–µ–љ–Є–µ
Cirrhosis is the destruction of normal liver tissue which is replaced with nonfunctioning scar tissue surrounding areas of functioning liver tissue and nodules of pathologic regeneration. The scar tissue and regenerative nodules compress portal tracts and cause portal hypertension with dilatation of varicose veins at the lower part of the esophagus, enlargement of the spleen and fluid accumulation in the abdomen (ascites). Spectrum of imaging findings of the cirrotic liver includes: 1. Changes of the liverТs margin; 2. Liver atrophy and hypertrophy; 3. Diffuse heterogeneity. The process of cirrhosis distorts the hepatic parenchyma. Although present in all patients with end-stage cirrhosis, this distortion has a variable effect on the configuration of the liverТs margin which may be smooth, nodular (fine to coarse Уcobble stoneФ margin with nodules < 3 cm), or grossly lobular (deformed by more than one nodule > 3 cm). Margins that are smooth or deformed by multiple small nodules are typical for micronodular cirrhosis, whereas a coarse nodularity of the margin is the result of macronodular cirrhosis. However, lobular livers are usually the resullt of marked subsegmental atrophy and hypertrophy rather than of large regenerative nodules (1). Approximately 25% of end-stage cirrhotic livers are normal in size and configuration; 36% are diffusely atrophic. Most of the remaining end-stage cirrhotic livers exhibit a combination of segmental atrophy and hypertrophy (1). Main cause of heterogeneity of the liver in CT and MR images is diffuse fibrosis. In our case the liverТs margin is nodular with nodules < 3 cm that are typical for macronodular cirrhosis, the liverТs size is normal. Diffuse fibrosis is clearly depicted in unenhanced CT and T1-weighted MR images as patchy, poorly defined region of low attenuation. In T2-weighted MR images fibrosis looks like some regions of high signal intensity of similar configuration as seen in unenhanced CT. Enlarged abdominal lymph nodes can be detected with CT in approximately 50% of patients. They are more common in the portacaval space and porta hepatis (2). Liver cirrhosis is the prime risk factor for hepatocarcinogenesis. Kubicka et al. showed that among patients with hepatocellular carcinoma 74.6% had liver cirrhosis (3). Moreover, Rodriguez et al. showed that the risk of hepatocellular carcinoma increased to 17% after 5 years of follow-up in patients with Child stage A or B cirrhosis (4).
–Ю–Ї–Њ–љ—З–∞—В–µ–ї—М–љ—Л–є –і–Є–∞–≥–љ–Њ–Ј
ћакронодул€рный цирроз печени
–Р–і—А–µ—Б —Б–ї—Г—З–∞—П –≤ –Є–љ—В–µ—А–љ–µ—В–µ
http://www.tomography.ru/cases.php?id=1
|
–†–Є—Б—Г–љ–Њ–Ї 1a 
–†–Є—Б—Г–љ–Њ–Ї 1b 
–†–Є—Б—Г–љ–Њ–Ї 1c 
–†–Є—Б—Г–љ–Њ–Ї 2a 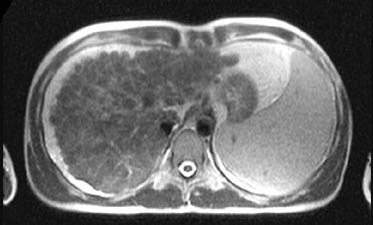
–†–Є—Б—Г–љ–Њ–Ї 2b 
–†–Є—Б—Г–љ–Њ–Ї 2c 
–†–Є—Б—Г–љ–Њ–Ї 2d 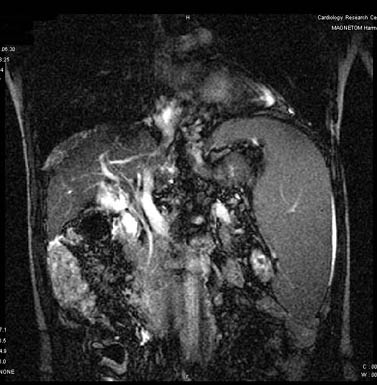
–†–Є—Б—Г–љ–Њ–Ї 2e 
|
